Steun het IDF Support IDF Steun het Diabetesfonds Check for Obesitas and Diabetes! Word bewust van Obesitas & Diabetes!
About: Dokter on line
· Snel · Voordelig · Discrete verzending . Erkende Artsen · Authentieke medicijnen · De grootste online -apotheek · Geen afspraak nodig · Vertrouwelijk en veilig · Geen wachtkamer · Bestel thuis of op het werk · 20% korting op sommige kosten voor trouwe klanten!
http://nl.dokteronline.com/669/coupon/C1070674/ Met de coupon code krijgt u extra 10 euro korting! Deze actie is alleen via deze blog, en nergens anders verkrijgbaar. Let op: als u naar bestellen gaat bij het product van uw keuze dan ziet u de korting onder COUPON rechts. U krijgt deze bovenop de al geldende acties en aanbiedingen! en profiteert dus dubbel!
Dubai International Convention and Exhibition Centre Sheihk Zayed Road Dubai, United Arab Emirates http://www.dicc.ae
Key dates
21 April 2010 - Call for topics close 1 September 2010 - Registrations open 1 February 2011 - Abstract submissions open 1 February 2011 - Grant applications open 20 April 2011 - Abstract submissions close 20 April 2011 - Grant applications close 1 August 2011 - Early registrations rate close 31 August 2011 - Late breaking abstract submissions close
0
1
2
3
4
5
- Gemiddelde waardering: 0/5 - (0 Stemmen) Categorie:organisations Tags:Diabetes World Congress
Geschiedenis
Geschiedenis
Al duizenden jaren vechten mensen tegen diabetes. Tot begin vorige eeuw was het hopeloos. Mensen gingen binnen een paar dagen of maanden dood aan diabetes type 1. Nog maar anderhalve eeuw weten we wat diabetes eigenlijk is. En pas sinds 1921 is een succesvolle behandeling mogelijk.
1500 v. Chr.
Diabetes duikt al op in oude geschriften uit India, Egypte en Griekenland. Het zijn beschrijvingen van mensen die lijden aan een geheimzinnige ziekte waardoor hun lichaam wegteert. Het valt op dat mieren en bijen afkomen op de zoete urine van de zieken. Men probeert van alles om de mensen te helpen: van kruidendrankjes, honing en wijn tot aderlaten. Niets helpt.
250 - 150 v. Chr.
De Griekse arts Apollonius van Memphis bedenkt de naam 'diabetes'. Het betekent letterlijk 'doorstroming', want het lijkt erop dat de patiënten meer vocht verliezen dan ze kunnen drinken. Men denkt zelfs dat hun lichaam langzaam wegsmelt. Vanwege de zoete urine wordt de naam later uitgebreid tot 'diabetes mellitus': honingzoete doorstroming.
Ca. 1000
Artsen in de hele wereld kennen diabetes, maar weten nog steeds niet wat ze eraan kunnen doen. Patiënten in Griekenland krijgen het advies veel paard te rijden om minder te hoeven plassen. In Europa probeert men het met aderlatingen en opium. Of met zoveel mogelijk eten, om maar niet te veel af te vallen.
Ca. 1800
De geleerden John Rollo en Claude Bernard ontdekken dat diabetespatiënten niet alleen te veel suiker in hun urine hebben, maar ook in hun bloed. Ze ontdekken ook dat diabetes te maken heeft met de suikerstofwisseling. Kort daarna beschrijft de onderzoeker Traube hoe het eten van koolhydraten invloed heeft op de bloedsuikerspiegel.
1869
Een doorbraak: de Duitse Paul Langerhans ontdekt in de alvleesklier cellen die insuline maken. Ze liggen in groepjes bij elkaar en lijken daarom op eilandjes. Deze sindsdien naar hem vernoemde 'eilandjes van Langerhans' maken insuline aan. Zonder insuline kan het lichaam geen suikers verwerken en ontstaat diabetes. Maar dat wordt pas twintig jaar later ontdekt, door Joseph von Mehring en Oskar Minkowski. Zij merken dat honden waarvan ze de alvleesklier weggehaald hebben, diabetes krijgen.
1921
Uiteindelijk lukt het Frederick Banting en Charles Best om insuline uit de alvleesklier van honden en kalveren te gebruiken voor mensen. De eerste patiënt die zij met succes behandelen is de 14-jarige Leonard Thompson. Hij leeft daarna nog dertien jaar in redelijke gezondheid. Banting krijgt de Nobelprijs voor deze ontdekking.
1950-1980
Met DNA-technieken wordt synthetische insuline ontwikkeld, waardoor geen insuline van bijvoorbeeld varkens meer nodig is.
1980 en verder
Met testjes en instrumenten kunnen diabetespatiënten nu zelf hun bloedsuikerspiegel testen. Dat geeft meer controle en flexibiliteit. Ook insulinesoorten en de methoden om ze in te spuiten worden flink verbeterd. Onderzoekers blijven zoeken naar manieren om diabetes te behandelen en mogelijk te genezen.
Er zijn veel vragen en misverstanden over diabetes. Hier ziet u enkele veel voorkomende fabels:
Van veel snoepen krijg je diabetes
Van alleen veel suiker eten krijg je niet zomaar diabetes. Door andere oorzaken gaat er in het lichaam wat mis. De alvleesklier produceert niet voldoende of zelfs helemaal geen insuline meer. Waarom dat gebeurt is nog een raadsel. Er zijn aanwijzingen dat sommige dingen een risico kunnen zijn. Suiker op zich vormt dus geen risico. Toch is het niet aan te raden om veel te snoepen. Want het is wel een feit dat in suikerrijke producten vaak ook meer vetten en calorieën zitten. Daarvan word je dik, en dat op zich kan weer wel leiden tot diabetes type 2. Mensen met een grotere kans op diabetes zijn mensen met fors overgewicht (vetophoping in de buikstreek), mensen met diabetes in de familie en vrouwen die zwangerschapsdiabetes hebben gehad. Wilt u meer weten? Er ligt een gratis informatiebrochure voor u klaar.
Zware diabetes / een beetje diabetes
Je hebt diabetes of je hebt het niet. Net als een beetje zwanger zijn: dat bestaat ook niet. Ieder mens met diabetes is anders. Daar wordt de behandeling ook op aangepast. Doel is om de natuurlijke situatie in het lichaam zoveel mogelijk te benaderen. Mensen met diabetes type 1 moeten meerdere keren per dag insuline spuiten omdat hun insulineproducerende cellen in de alvleesklier weg zijn. Mensen met diabetes type 2 hebben op zich die cellen nog wel, maar ze werken niet meer goed of het lichaam reageert niet meer goed op de insuline. Zij krijgen meestal tabletten om de alvleesklier te stimuleren meer insuline aan te maken, of om de lichaamscellen de insuline beter te laten gebruiken. Wilt u meer weten over diabetes? Vraag de gratis informatiebrochure aan!
Mensen met diabetes mogen geen suiker
Het is een fabeltje dat mensen met diabetes geen suiker mogen. Ons voedsel wordt door het lichaam omgezet in onder meer glucose (suiker) wat vervolgens aan het bloed wordt afgegeven. Dus ook een droog biscuitje of een aardappel wordt deels omgezet in suiker. Het is daarom niet nodig om suikervrije producten te kopen. Iemand met diabetes mag wel suiker, maar met mate. De persoon kan dan zelf uitmaken waar hij de suiker uit haalt.
Alleen oude mensen krijgen diabetes
Nee, steeds meer mensen van alle leeftijden krijgen diabetes. Vooral diabetes type 2, die samenhangt met een ongezondere levensstijl en overgewicht. Er zijn in Amerika zelfs al kleuters die het hebben! Maar ook steeds meer kinderen en jongeren krijgen diabetes type 1. Onderzoekers zijn druk bezig met uitzoeken hoe dat komt.
Diabetes is besmettelijk
Je kunt niet door contact met iemand anders diabetes krijgen. Diabetes is geen infectieziekte, die door bacteriën, virussen of lichamelijk contact kan worden overgedragen. Ook niet via borstvoeding. Diabetes is een 'technisch' probleem van het lichaam dat door oorzaken binnen het eigen lichaam ontstaat.
Je kunt van diabetes genezen
Nee, diabetes is momenteel nog niet te genezen. Het dichtst in de buurt van genezing komt transplantatie van de alvleesklier, bij mensen met diabetes type 1. Maar dat is een zware ingreep met ook daarna de nodige risico’s vanwege onder andere de anti-afstotingsmedicijnen die iemand de rest van zijn leven moet slikken. Transplantatie wordt dan ook alleen uitgevoerd bij mensen die door diabetescomplicaties in levensgevaar zijn, zoals uitval van de nieren (in combinatie met een niertransplantatie).
Technisch gezien heeft iemand daarna geen diabetes meer, want het lichaam maakt zelf weer insuline aan. Wel bestaan in het hele lichaam nog steeds de schadelijke gevolgen ervan. Een andere mogelijkheid is transplantatie van de insulineproducerende cellen uit de alvleesklier (de eilandjes van Langerhans). De resultaten zijn nog wisselend en veel onderzoek wordt gedaan om de techniek te verbeteren. Mensen met diabetes type 2 hebben geen baat bij transplantatie, omdat hun hele lichaam ongevoeliger is geworden voor insuline.
Soms kan iemand met diabetes type 2 wel met gezond leven zijn bloedsuikerspiegel binnen normale grenzen houden. Maar dat wil niet zeggen dat hij geen diabetes meer heeft. De diabetes is alleen goed onder controle. Als die persoon even wat minder oplet met eten, stijgen de bloedglucosewaarden weer snel.
Iemand met diabetes is ziekelijk
Nee, iemand met diabetes die goed behandeld wordt en geen ernstige diabetescomplicaties heeft, kan in principe gewoon fit door het leven. Je bent niet opeens een ‘zwak’ persoon omdat je diabetes hebt. Ook heb je dezelfde kans op verkoudheid en griep als iedereen. Maar áls je met diabetes een virusinfectie zoals een griep hebt, kan dat wel heel vervelend zijn voor het onder controle houden van de bloedsuiker. Infecties kunnen net als emoties en stress de bloedsuikerspiegel uit balans brengen. Daarnaast heeft het lichaam door diabetes vaak meer moeite om een infectie te overwinnen. Daarom krijgen mensen met diabetes het advies om een griepprik te halen.
The International Diabetes Federation (IDF) is an umbrella organization of over 200 national diabetes associations in more than 160 countries. It represents the interests of the growing number of people with diabetes and those at risk. The Federation has been leading the global diabetes community since 1950. IDF’s mission is to promote diabetes care, prevention and a cure worldwide. Led by the International Diabetes Federation, the Unite for Diabetes campaign secured a United Nations Resolution on diabetes in December 2006. The Federation continues to lead the global effort to implement Resolution 61/225 under the Unite for Diabetes banner.
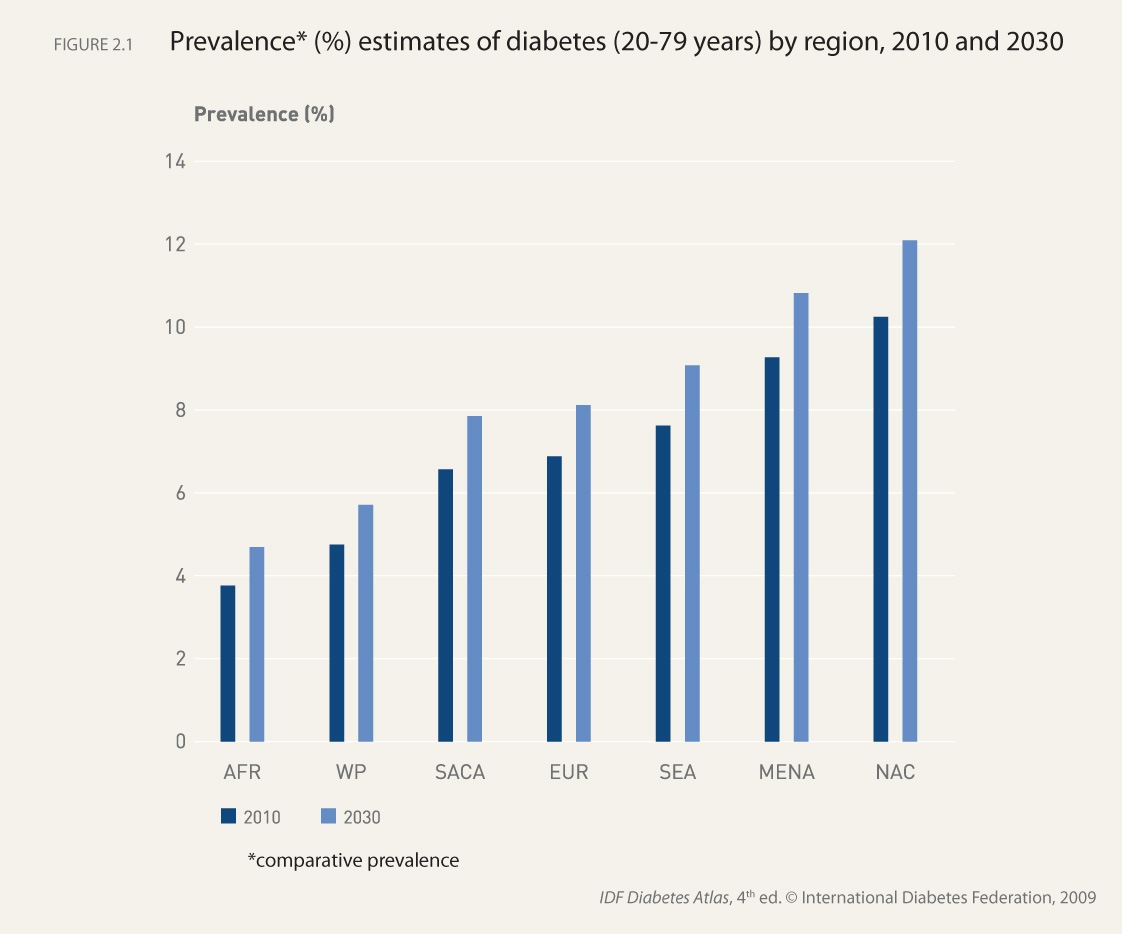
The Federation is engaged in action to tackle diabetes from the local to the global level―from programmes at community level to worldwide awareness and advocacy initiatives. The Federation is divided into seven regions, with the aim of strengthening the work of national diabetes associations and enhancing the collaboration between them. The Federation’s national diabetes associations are divided into the following seven regions: Africa (AFR), Europe (EUR), Middle East and North Africa (MENA), North America and Caribbean (NAC), South and Central America (SACA), South-East Asia (SEA) and Western Pacific (WP). The Federation’s activities aim to influence policy, increase public awareness and encourage health improvement, promote the exchange of high-quality information about diabetes, and provide education for people with diabetes and their healthcare providers. IDF is associated with the Department of Public Information of the United Nations and is in official relations with the World Health Organization (WHO) and the Pan American Health Organization (PAHO).
IDF Executive Office
International Diabetes Federation (IDF) Chaussée de la Hulpe 166 B-1170 Brussels, Belgium Tel: +32-2-5385511 l Fax: +32-2-5385114 Email: info@idf.org Website: www.idf.org
Er zijn verschillende soorten diabetes, naast de bekende vormen diabetes type 1 en type 2. De andere vormen lijken wel vaak sterk op diabetes type 1 of type 2, of zijn er eigenlijk een vorm van. Waarschijnlijk worden in de toekomst nog meer soorten diabetes ontdekt, als meer genetisch onderzoek mogelijk is.
De verschillende soorten diabetes hebben verschillende oorzaken en meestal ook een eigen behandeling.
MODY: een vorm van diabetes die aanvankelijk kan lijken op diabetes type 2. > Meer over MODY
LADA: een soort diabetes type 1 die zich juist vermomt als diabetes type 2. > Meer over LADA
MIDD: een zeldzame vorm van diabetes die samengaat met doofheid en via de moeder overerft. > Meer over MIDD
Neonatale diabetes: een vorm van diabetes die bij baby's jonger dan zes maanden ontstaat. > Meer over neonatale diabetes
Diabetes insipidus: bij deze soort diabetes draait het niet om bloedsuiker, maar om vocht. Het heeft niets te maken met 'suikerziekte'. > Meer over diabetes insipidus
De mogelijke bijkomende gevolgen van MODY, LADA, MIDD en neonatale diabetes zijn hetzelfde als voor diabetes type 1 of type 2.
nuttige links voor mensen met diabetes, of mensen die hun leefstijl willen verbeteren.
De Diabetesvereniging Nederland (DVN) is de grootste patiëntenvereniging van Nederland. De mensen die zich voor deze vereniging inzetten, verstrekken informatie over diabetes, geven educatieve cursussen, behartigen de belangen van diabeten, regelen symposia en bemannen de diabetesposten. www.dvn.nl/
www.mijndvn.nl kan iemand met diabetes een persoonlijk profiel inrichten, waarop alle functionaliteiten voor goede diabeteszorg te vinden zijn. Voordeel van deze pagina is dat iemand met diabetes vanuit een pagina alle zorg kan organiseren die nodig is voor een goede gezondheid. Gratis voor de gebruiker.
Het diabetesforum is het drukst bezochte forum in Nederland en veel mensen hebben steun aan het lotgenotencontact.
www.cyberpoli.nl Deze website is een online vraagbaak waar kinderen en jongeren met diabetes en hun ouders ieder moment van de dag en kosteloos vragen kunnen stellen aan een panel van deskundigen. De website is opgezet door Stichting Artsen voor Kinderen, een organisatie die kwaliteit van leven wil verbeteren van kinderen met een chronische ziekte.
Nnationaal centrum voor de behandeling van kinderen met diabetes: www.diabeter.nl
De Bas van de Goor Foundation heeft als missie om de kwaliteit van leven voor mensen met diabetes te verhogen door middel van sport. Voornamelijk voor kinderen met diabetes. Meer informatie op www.basvandegoorfoundation.nl
Ontmoetingsplek met informatie en activiteiten voor jong volwassenen met type 1 diabetes. http://www.diabetenweten.nl/www.diep.info/ is een handige site voor mensen met type 2 diabetes. Met allerlei informatie over type 2 diabetes, bloedglucosewaarden, leefstijl, behandeling, zelfcontrole en leven met diabetes.
Het Diabetescentrum van het VU medisch centrum in Amsterdam heeft een informatieve website, met algemene wetenswaardigheden over diabetes en de behandeling. www.diabetescentrum.nl
Novo Nordisk probeert wereldwijd het diabetes probleem onder de aandacht te brengen. Meer hierover leest u op www.changingdiabetes.nl/. Ook onder jongeren komt diabetes steeds vaker voor. Informatie over diabetes en jongeren kunt u vinden op www.youngvoicestv.nl/.
Website van farmaceut Nefarma over de rol van geneesmiddelen in de afgelopen 20- 30 jaar voor verschillende aandoeningen, waaronder diabetes. Met informatie over geneesmiddelen, de invloed daarvan op de kwaliteit van leven, brochures over de aandoeningen en een interview met een patiënt. http://www.wewordensteedsbeter.nl/cms/publish/content/showpage.asp?pageid=3129
Op de site van het Voedingscentrum staat veel informatie vinden over voeding, gewicht en gezond eten. Ook voor lekkere en gezonde recepten. www.voedingscentrum.nl/
De site van de Nederlandse Diabetes Federatie geeft informatie over de richtlijnen voor diabeteszorg en de diabetespas. Dat is een handig hulpmiddel om zelf je diabetescontroles in de gaten te houden. De website is vooral voor professionals in de gezondheidszorg. www.diabetesfederatie.nl/
Op het Diabetesplein staat veel informatie bij elkaar over diabetesonderwerpen, zoals behandeling, en op reis gaan met diabetes. www.diabetesplein.nl/
Over pijnklachten ten gevolge van diabetische neuropathie, ook wel ‘zenuwpijn’ genoemd. Deze pijnklachten komen bij circa 25% van de diabetespatiënten voor. Zie www.stopdepijn.nl/ voor patiënten en hun omgeving.
Veel mensen met diabetes krijgen last van hun maag en darmen. Door beschadigde zenuwen kan de maagontlediging niet meer goed werken. Dat geeft vaak een opgeblazen, verstopt gevoel. Voor meer informatie over de behandeling van maag- en darmproblemen, zie de Maag Lever Darm Stichting, www.mlds.nl/.
Enkele mensen met diabetes krijgen door ernstige vaatproblemen te maken met een amputatie. Voor meer informatie over het omgaan met, de behandeling en nazorg van amputatie, zie de Landelijke Vereniging van Geamputeerden, www.lvvg.nl
Informatie over erfelijkheid van diabetes en andere aandoeningen: www.erfelijkheid.nl/
Via de Diabetesvereniging Nederland (www.dvn.nl/) kun je informatieve video’s aanschaffen in diverse buitenlandse talen, die ook speciaal gericht zijn op mensen uit die betreffende culturen. Ze zijn verkrijgbaar in het Arabisch, Berber, Turks, Marokkaans, Hindoestaans en Antilliaans.
De American Diabetes Association geeft veel goede informatie (in het Engels) op www.diabetes.org/.
Stivoro: onder andere informatie over stoppen met roken www.stivoro.nl/ of bel 0900 – 9390
www.spreekuurthuis.nl/themas bevat veel informatie over diabetes type 1 en type 2 en allerlei andere aandoeningen.
www.hospi-taal.nl/ Informatie voor mensen met diabetes: informatie folders, multiple choice quizen en medische animaties.
www.diabetesoogzorg.nl/ Informatie over diabetes en alle oogheelkundige aspecten rondom diabetes en oogzorg.
0
1
2
3
4
5
- Gemiddelde waardering: 0/5 - (0 Stemmen) Categorie:organisaties Tags:nuttige links voor mensen met diabetes en mensendie hun leefstijl willen verbeteren
Wat is diabetes
Wat is diabetes
Diabetes wordt ook wel 'suikerziekte' genoemd.
De officiële naam is diabetes mellitus.
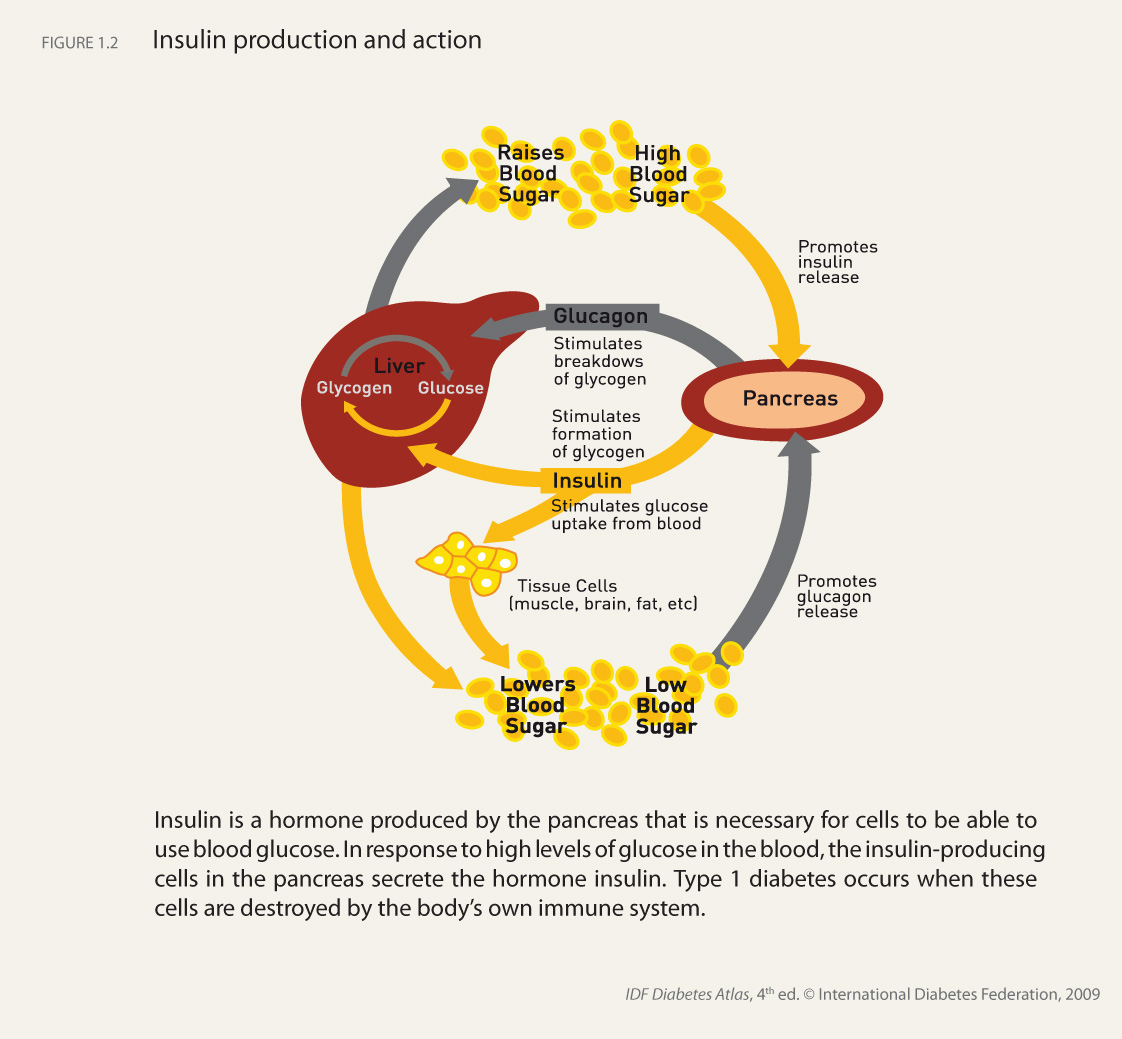
Bij diabetes kan het lichaam de bloedsuiker niet meer zelf in evenwicht houden. Normaal regelt het lichaam de bloedsuikerspiegel heel nauwkeurig, met het hormoon insuline. Mensen met diabetes maken zelf geen insuline meer, of hun lichaam reageert niet meer op de insuline. Dat hangt af van de soort diabetes.
Als insuline zijn werk niet kan doen, loopt de bloedsuiker veel te hoog op. Als er lange tijd te veel suiker in het bloed zit, is dat erg ongezond. Daarom is het belangrijk om diabetes zo snel en goed mogelijk te behandelen. Naast het probleem met bloedsuiker, zijn ook vaak het cholesterol en de bloeddruk te hoog.
Bloedsuiker
Bloedsuiker heet officieel 'bloedglucose'. Geen mens kan zonder glucose, want die geeft het lichaam energie waardoor alle spieren en organen werken. Glucose komt uit koolhydraten in de voeding.
Koolhydraten zitten niet alleen in zoete dingen, zoals suiker en fruit, maar ook in sommige groenten, melk, brood en aardappelen en andere soorten zetmeel. Van koolhydraten maakt het lichaam glucose; die komt in het bloed terecht als bloedsuiker en gaat naar alle lichaamscellen voor energie. Maar te veel is niet goed.
Normaal zorgt het lichaam ervoor dat er precies genoeg insuline vrijkomt om de hoeveelheid glucose in het bloed te verwerken. Zo blijft de bloedsuikerspiegel altijd binnen bepaalde grenzen. Bij diabetes is dat evenwicht weg.
Insuline is onmisbaar
Insuline wordt gemaakt in de alvleesklier. Wanneer geen of onvoldoende insuline wordt gemaakt, of als het lichaam niet meer reageert op insuline, heeft het lichaam moeite om glucose uit het bloed te krijgen. De bloedsuiker blijft dan rondstromen en kan niet gebruikt worden voor energie. Het gevolg is erge dorst en veel plassen. Want het lichaam probeert om de glucose op een andere manier kwijt te raken. Doordat iemand geen glucose, dus geen energie kan opnemen, voelt hij zich moe.
Although guidelines for best practice in diabetes care are readily available, including the IDF Global Guideline on Type 2 Diabetes, and there are several frameworks to guide their implementation, it remains a challenge in all countries to bridge the gap between actual and optimal care.
Investments in education and change
One important part of any solution is education. Diabetes-specific education is required for healthcare personnel and people with diabetes; and in addition training is needed to help them integrate new knowledge and transform old practices. The latter is essential if clinical outcomes for people with diabetes are to be improved. It has been shown that without a purposeful, planned method of changing clinical or personal behaviour, very little happens. Investment must be made not only to ensure specialized diabetes education is accessible to healthcare personnel and people with diabetes but also to ensure both groups are trained in how to implement change 1 2 .
Ministries of Health and health administrators need to recognize and give support to the special healthcare needs of people with diabetes 1 and this includes designing health systems that facilitate best practice 2 . Providing good diabetes care for a population requires the coordination of the health systems across three levels. At the centre of all care is the person with diabetes, their family and their immediate carers. At the middle level is the community and healthcare organizations within which care is delivered. Effective functioning across the providers needed to care for people with diabetes requires supporting policy and financial frameworks. The World Health Organisation’s Innovative Care for Chronic Conditions Framework 3 provides guidance on the relationships between, and the contents of, these three levels. This framework was designed to be helpful within different resource settings, rich to poor, and has been developed with suggested methods of quality improvement to incrementally strengthen health systems for diabetes and other chronic diseases (see Beyond Access to Insulin).
Modern improvement processes have had positive results in many countries, including Canada, USA, United Kingdom, Ghana, Malawi, South Africa, Russia and Peru. A critical factor in their success is that they develop and implement solutions specific to the realities of their settings 2 . Reorganization of current resources or addition of new resources may be required to fill overt gaps in care, such as interdisciplinary teams specially trained to provide diabetes self-management education and follow-up or access to essential medicines packaged with education to support their use. The advancement of diabetes care relies not only on increased knowledge and behaviour change but also on using proven methods to advance health systems to support best practice 4 .
Self-management education and support
"Diabetes self-management education (DSME) and ongoing self-management support are critical components of effective diabetes care, and significant contributors to metabolic and psychological outcomes." 5 In many areas of the world people with diabetes cannot access this essential treatment. Interactive DSME is essential for people with diabetes to understand their condition, protect themselves from harm and make lifestyle changes to optimize their health. To design an accessible programme, funding needs to be provided for healthcare personnel with specialized training in DSME. Programmes must be locally affordable, offered in areas accessible to the target population, delivered at appropriate literacy levels and be culturally relevant. Diabetes self-management education and diabetes self-management support must be available and accessible for people with diabetes if optimal outcomes are to be achieved 5 .
People with diabetes have the right to understand their disease, make informed choices and receive care based on best practice. They must be part of the team that manages their condition.This can only be achieved if interdisciplinary teams and people with diabetes have the information and tools to make changes based on best practice and recognized improvement strategies are used to support meaningful system change.
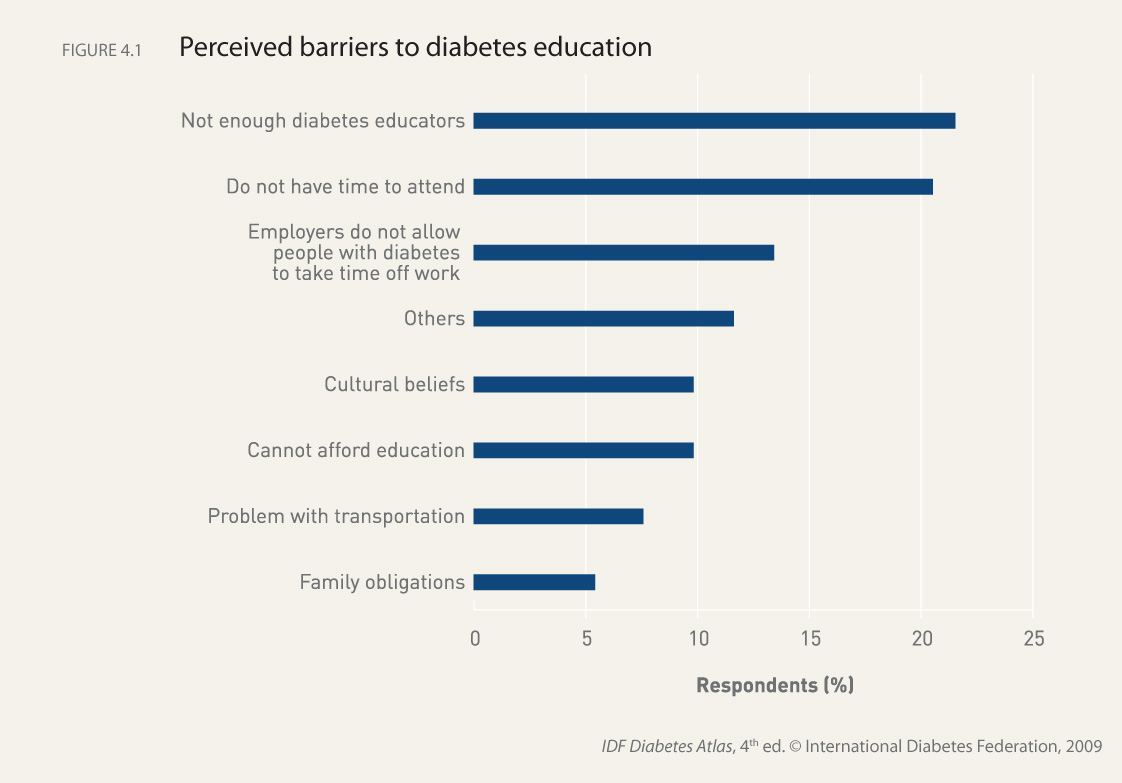
Text box 4.4 Survey on diabetes education practices
A survey was carried out by the IDF Consultative Section on Diabetes Education in 2008 to gain a deeper appreciation for diabetes education practices worldwide and to provide a preliminary look at diabetes education in specific areas. The purpose of the survey was to capture responses from providers regarding practice setting, descriptions of diabetes teams, resources for diabetes education, community services and barriers to diabetes education.
The survey questionnaire was based on the structural and process standards for diabetes health education defined in the IDF’s International Consensus Standards for Diabetes Education 6 , which provide a benchmark against which the quality of DSME programmes can be evaluated.
The surveys were completed by healthcare professionals selected to participate in train-the-trainer sessions. The survey respondents represented healthcare institutions in the IDF African, European, Middle East and North African, North America and Caribbean, and South and Central American Regions.
Survey results
The survey results provide preliminary data on the status of diabetes education in the different regions. Forty-five out of 55 participants responded, giving a response rate of 82%. Respondents represented 26 countries in the five regions.
The results indicated that diabetes education was integrated into national diabetes programmes in two-thirds of the countries which had such a programme. The results also showed that diabetes education was practised in a variety of settings by many different healthcare providers. When asked about the most significant barriers to diabetes education, lack of resources in terms of the number of diabetes educators from the systems perspective was most often cited (see Figure 4.1). Another important barrier was that people with diabetes did not have time or support from employers to pursue diabetes education. The results also confirm that despite the presence of national diabetes programmes, people with diabetes may not have access to adequate education and care.
These data are limited by the sample chosen to participate and should not be considered statistically representative. However, the respondents do provide insight into their perception of diabetes education in their country. Despite the limitations of the survey, the results demonstrate a clear need for increased numbers of diabetes educators and support for diabetes self-management education for people with diabetes.
1: World Health Organization. Innovative Care for Chronic Conditions: Building Blocks for Action. Global Report. Geneva: World Health Organization; 2002. http://www.who.int/diabetesactiononline/about/icccreport/en/ 2: Cabana MD, Rand CS, Powe NR, et al. Why don't physicians follow clinical practice guidelines? A framework for improvement. JAMA 1999; 282 (15): 1458-1465. 3: Jordan EJE, Pruitt SD, Bengoa R, et al. Improving the quality of health care for chronic conditions. Quality and Safety in Health Care 2004; 13 (4): 299-305. 4: World Health Organization. 2008-2013 Action Plan for the Global Strategy for the prevention and control of non-communicable disease. Geneva: World Health Organization; 2008. www.who.int/nmh/Actionplan-PC-NCD-2008.pdf 5: Berwick DM. Lessons from developing nations on improving health care. BMJ 2004; 328 (7448): 1124-1129. 6: IDF Consultative Section on Diabetes Education International Consensus Standards for Diabetes Education 2003
The ultimate goal of diabetes therapy is to prevent diabetes complications, such as kidney and heart diseases, in order to improve quality of life and life expectancy. There is excellent evidence that the development of complications can be significantly reduced and their progress and impact limited once they have developed 1 .
Tailoring approaches to the person with diabetes
On a day to day basis most decisions that affect the risk of complications are made by people with diabetes themselves, not by health professionals. Therefore, structured diabetes education to empower people with diabetes, and their carers, to manage their condition is crucial (see Diabetes Education). Lifestyle measures such as eating healthily, maintaining a normal weight, regular physical activity, and not smoking are central to diabetes management, and could lead to improvements in blood glucose, lipids and blood pressure and a reduced risk of complications. In addition, medication often has an important role to play, particularly for the control of blood glucose, lipids and blood pressure.
The IDF Global Guideline for Type 2 Diabetes 1 provides an evidence-based framework for setting targets for glucose, blood pressure and lipids, and titrating treatment in order to achieve them. Oral glucose lowering medication is prescribed when lifestyle measures are insufficient to achieve blood glucose control. For most people metformin, which increases sensitivity to insulin, is the drug of first choice followed by a sulfonylurea, which stimulates insulin release. These drugs have been used in the management of diabetes for decades. If these drugs fail to control blood glucose then other options include thiazolidinediones (increase sensitivity to insulin) and alpha glucosidase inhibitors (decrease rate of glucose absorption from the gut). Newer options include the so-called GLP-1 (glucagon-like peptide) mimetics and DPP-4 (dipeptidyl peptidase 4) inhibitors, both of which increase insulin release. At this time experience with these newer agents is limited but they may have a more prominent role in the future.
Overtime the insulin-producing cells within the pancreas of people with type 2 diabetes deteriorate and eventually in most people insulin is needed as other measures are not sufficient to control blood glucose. Insulin analogues may offer some advantages, particularly with respect to hypoglycaemia and weight gain. The introduction of insulin requires close cooperation between the person with diabetes and health carers.
Tailoring approaches to the resources available
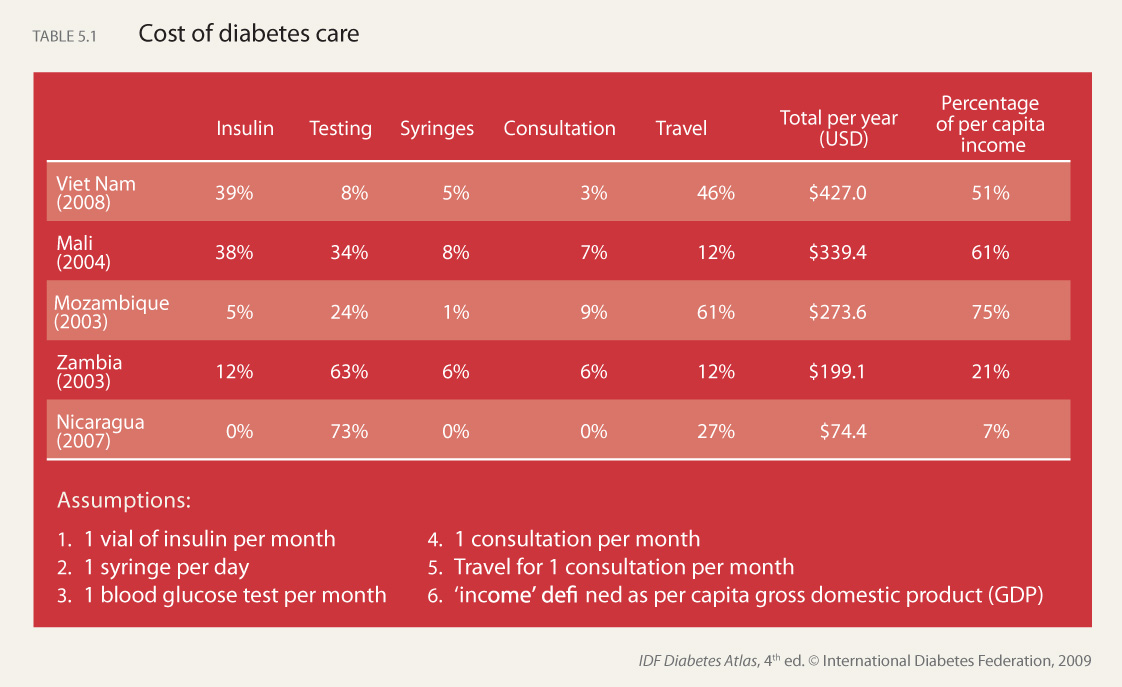
Diabetes care does not need to be expensive to be highly effective. In work carried out for the World Bank and World Health Organization 2 interventions for diabetes were classified into three levels based on an assessment of their feasibility and cost effectiveness in developing country settings. Interventions in the first level were found to be highly cost effective or even cost saving, and included moderate blood glucose and blood pressure control and foot care. Recognizing that most people with diabetes live in developing countries, the IDF Global Guideline provides guidance appropriate to three different levels of resource availability.
Screening for undetected diabetes
Type 2 diabetes has a long asymptomatic phase, which frequently goes undetected but during which diabetes complications are developing, and can be present in half or more people with diabetes at diagnosis. Thus, early detection and treatment could help reduce the burden of diabetes complications, and evidence suggests that earlier intensive treatment is indeed effective. However, issues such as who to screen, and what to do with those found to be at high risk of developing diabetes are unresolved. The solutions to these issues will differ between countries, dependent on factors that include the prevalence of undiagnosed diabetes, and the available healthcare resources.
The background paper, Challenges of Type 2 Diabetes, on which this summary is based is available in the Downloads section.
Box 4.3 Areas of individual diabetes care requiring regular review
Assessment topic
Self-care knowledge and beliefs
Lifestyle adaptation and wishes (including nutrition, physical activity, smoking)
Psychological status
Self-monitoring skills and equipment
Body weight trends
Blood glucose control
Blood pressure control
Blood lipid control
Cardiovascular risk
Neuropathy
Erectile dysfunction
Foot condition
Eyes
Kidneys
Pre-pregnancy advice (as appropriate)
Medication review
1: International Diabetes Federation. Global Guideline for Type 2 Diabetes. Brussels: International Diabetes Federation; 2005. http://www.idf.org/node/1285?unode=B7462CCB-3A4C-472C-80E4-710074D74AD3 2: Narayan KV, Kanaya PZA, Williams D, et al. Diabetes: The Pandemic and Potential Solutions. In Jamison D, Breman J, Measham A, et al, editors. Disease control priorities in developing countries.Second Edition. World Bank/Oxford University Press; 2006. p591-604.
0
1
2
3
4
5
- Gemiddelde waardering: 0/5 - (0 Stemmen) Categorie:what is diabetes Tags:The Challenges of Type 2 Diabetes
The Prevention of Type 2 Diabetes
The Prevention of Type 2 Diabetes
There is excellent evidence that type 2 diabetes can be prevented, or at least its onset delayed, in individuals at high risk. Most of the evidence is from studies that have included people with IGT. Behavioural modification and pharmacological interventions have both been shown to be effective, and to reduce the onset of new diabetes by up to 60% or more. Overall the evidence suggests that lifestyle counselling to support behavioural change, such as losing weight (for those overweight), increasing physical activity, and eating a healthy diet is more effective than pharmacological interventions 1 . For example, for around every six people at high risk treated with lifestyle counselling one new case of diabetes will be prevented over five years, whereas to prevent one new case with an oral diabetes drug, around 11 people will need to be treated. There is evidence that the lower risk of diabetes from lifestyle counselling persists long after its discontinuation, with results from a study in China showing that the benefits were still apparent 20 years later.
Translating findings from prevention trials into the community
The challenge now is to translate the findings from the well resourced research studies into diabetes prevention initiatives that are affordable and feasible in both low- and high-income countries. The challenge includes finding the most efficient and cost-effective ways to identify people at high risk of developing diabetes, and then providing an effective intervention that is feasible and affordable within the local setting. While there are examples of such initiatives they have tended to be small and poorly evaluated. It is also clear that an initiative developed for one population or group may not be appropriate for another population or group. Thus, community initiatives aimed at the prevention of type 2 diabetes in individuals at high risk need to be developed and evaluated for the specific settings in which they will be used.
National efforts to prevent diabetes
It is acknowledged that while it is important to identify individuals at high risk of developing diabetes for preventive efforts, this will have a limited impact on the rate of diabetes at a national level. What are also needed are measures that reduce the risk across the whole population. Evidence suggests that relatively small improvements in nutrition, reductions in obesity and increases in physical activity if applied across a whole population can have a large impact on the rates of diabetes, and other chronic diseases that share the same risk factors (such as cardiovascular disease and many cancers). Much more attention needs to be given as to how to achieve such population-wide changes. The DEHKO project in Finland 2 provides an example of a comprehensive approach to diabetes prevention and management, which aims to improve nutrition and physical activity across the population, identify and provide individualized support to those at high risk of diabetes and assist with the early detection and management of those who actually have diabetes (see Box 4.2).
Cost effectiveness of prevention
Economic evaluations of approaches to identifying and providing preventive measures to people at high risk of diabetes generally suggest that these are cost effective. However, most evaluations contain many uncertainties and there is a need for further work to examine the cost effectiveness of interventions in everyday practice. There is an even greater challenge in assessing the cost effectiveness of population-wide measures.
The background paper, The Prevention of Type 2 Diabetes, on which this summary is based is available in the Downloads section.
Box 4.1 National Diabetes Prevention Plans 3
Government initiatives should include: • Advocacy —Supporting national associations and non-government organizations —Promoting the economic case for prevention • Community support —Providing education in schools on nutrition and physical activity —Promoting opportunities for physical activity through urban design (e.g. to encourage cycling and walking) —Supporting sports facilities for the general population • Fiscal and legislative —Examining food pricing, labelling and advertising —Enforcing environmental and infrastructure regulation (e.g. urban planning and transportation policy to enhance physical activity) • Engagement of private sector —Promoting health in the workplace —Ensuring healthy food policies in food industry • Media communication —Improving level of knowledge and motivation of the population (press, TV and radio)
Box 4.2 Examples of Prevention Programmes
Finland
The Development Programme for the Prevention and Care of Diabetes in Finland (DEHKO 2000–2010) 2 was the first national diabetes programme to implement strategies for the prevention of type 2 diabetes on a population-wide scale. It is now in its final phase after nearly a decade of activity, but there are further plans for the future. DEHKO is a programme that is widely watched for the comprehensiveness in which it has worked towards reducing the incidence of type 2 diabetes in a population and, at the same time, raising the quality of diabetes care.
The FIN-D2D Project (2003–2008) within DEHKO and the follow-up project to D2D are specifically tasked with the implementation of the prevention programme for type 2 diabetes. The FIN-D2D Project has also developed new models for prevention to be disseminated to all primary healthcare centres and occupational healthcare units in Finland. The effectiveness and the cost-effectiveness of these new prevention and care practices are being evaluated. The project is now working towards making the prevention of diabetes and cardiovascular disease part of healthcare routine. More information on DEHKO, which is coordinated by the Finnish Diabetes Association, is available at www.diabetes.fi.
Latin America
A project to reduce the burden of type 2 diabetes by education and lifestyle interventions in people at high risk is currently underway in Latin America. The LATIN_PLAN project will implement an intervention programme at primary healthcare level in Argentina, Brazil, Colombia, Ecuador, Peru, Uruguay and Venezuela.
The project is based on current evidence and best practice in the prevention of type 2 diabetes, especially those found in the European diabetes prevention projects (DE-PLAN and IMAGE projects). It also will develop and implement a curriculum for training diabetes prevention managers in Latin America, who will provide a basis for long-term activities at population level, and guarantee sustainability and continuity at the community level. The project is coordinated by the Research Unit of the Hospital Universitario La Paz in Madrid, Spain. More information is available from de_plan@ceiis.e.telefonica.net.
1: Gillies CL, Abrams KR, Lambert PC, et al. Pharmacological and lifestyle interventions to prevent or delay type 2 diabetes in people with impaired glucose tolerance: systematic review and meta-analysis. BMJ 2007; 334 (7588): 299. 2: Finnish Diabetes Association. Development Programme for the Prevention and Care of Diabetes in Finland DEHKO 2000-2010. 2009. http://www.diabetes.fi/sivu.php?artikkeli_id=831 3: Alberti KG, Zimmet P, Shaw J. International Diabetes Federation: a consensus on Type 2 diabetes prevention. Diabet Med 2007; 24 (5): 451-463.
Type 1 diabetes is rapidly increasing in children and adolescents in many countries, and evidence suggests that in a growing number of countries type 2 diabetes is now also being diagnosed in childhood.
Challenges of type 1 diabetes in children
Type 1 diabetes is one of the most common endocrine and metabolic conditions in childhood, and incidence is rapidly increasing especially among the youngest children. Insulin treatment is life-saving and lifelong. Self-discipline and adherence to a balanced diet are necessary if the disease is to be well managed. In many countries, especially in less privileged families, access to self-care tools and also to insulin is limited and this may lead to severe handicap and early death in children with diabetes.
Many children and adolescents find it difficult to cope emotionally with their condition. Diabetes causes them embarrassment, results in discrimination and limits social relationships. It may impact on school performance and family functioning. The financial burden may be aggravated by the costs of treatment and monitoring equipment.
Trends in incidence
Two international collaborative projects, the Diabetes Mondiale study (DiaMond) 1 and the Europe and Diabetes study (EURODIAB) 2 have been instrumental in monitoring trends in incidence through the establishment of population-based regional or national registries using standardized definitions, data collection forms and methods for validation.
The incidence of childhood onset type 1 diabetes is increasing in many countries in the world, at least in the under 15-year age group. There are strong indications of geographic differences in trends but the overall annual increase is estimated to be around 3%. There is evidence that incidence is increasing more steeply in some of the low prevalence countries such as those in central and eastern Europe. Moreover, several European studies have suggested that, in relative terms, increases are greatest in young children. There are clear indications that similar trends exist in many other parts of the world, but in sub-Saharan Africa incidence data are sparse or non–existent. Special efforts must be made to collect data, especially in those countries where diagnosis may be missed or neglected and, as a result, children die because they do not receive insulin.
Prevalence of type 1 diabetes in children
It is estimated that annually some 76,000 children aged under 15 years develop type 1 diabetes worldwide. Of the estimated 480,000 children with type 1 diabetes, 24% come from the South-East Asian Region, but the European Region, where the most reliable and up-to-date estimates of incidence are available, comes a close second (23%) (see Figure 2.4).
The continued mapping of global trends in incidence and prevalence of type 1 diabetes in all age groups, through use of data from existing and new registries, is thus important, and in conjunction with other scientific research may provide a logical basis for intervention studies and future primary prevention strategies which must be the ultimate goal.
The background paper, Diabetes in the Young, and country by country estimates on which the summary on type 1 diabetes in the young is based are available in the Downloads section.
Type 2 diabetes in the young
Type 2 diabetes in children and adolescents is on the increase in all countries, whether poor or rich. As with type 1 diabetes, many children with type 2 diabetes risk developing complications at an early age, which would place a significant burden on the family and society. There is growing recognition that type 2 diabetes in the young is becoming a global public health issue with a potentially serious health outcome 3 , in spite of the paucity of information in this area. A review of studies on type 2 diabetes in the young is available in the Diabetes Atlas, third edition 4 .
Map 2.4 New cases of type 1 diabetes in children, 0-14 years (cases per 100,000 aged 0-14 years per year), 2010
1: D.I.A.M.O.N.D. Project Group. Incidence and trends of childhood Type 1 diabetes worldwide 1990-1999. Diabet Med 2006; 23 (8): 857-866. 2: Patterson CC, Dahlquist GG, Gyürüs E, et al. Incidence trends for childhood type 1 diabetes in Europe during 1989-2003 and predicted new cases 2005-20: a multicentre prospective registration study. Lancet 2009; 373 (9680): 2027-2033. 3: Fagot-Campagna A, Narayan KM, Imperatore G. Type 2 diabetes in children. BMJ 2001; 322 (7283): 377-378. 4: International Diabetes Federation. The Diabetes Atlas.Third Edition. Brussels: International Diabetes Federation; 2006.
0
1
2
3
4
5
- Gemiddelde waardering: 0/5 - (0 Stemmen) Categorie:what is diabetes Tags:Diabetes in the Young: a Global Perspective
Diabetes and Impaired Glucose Tolerance
Diabetes and Impaired Glucose Tolerance
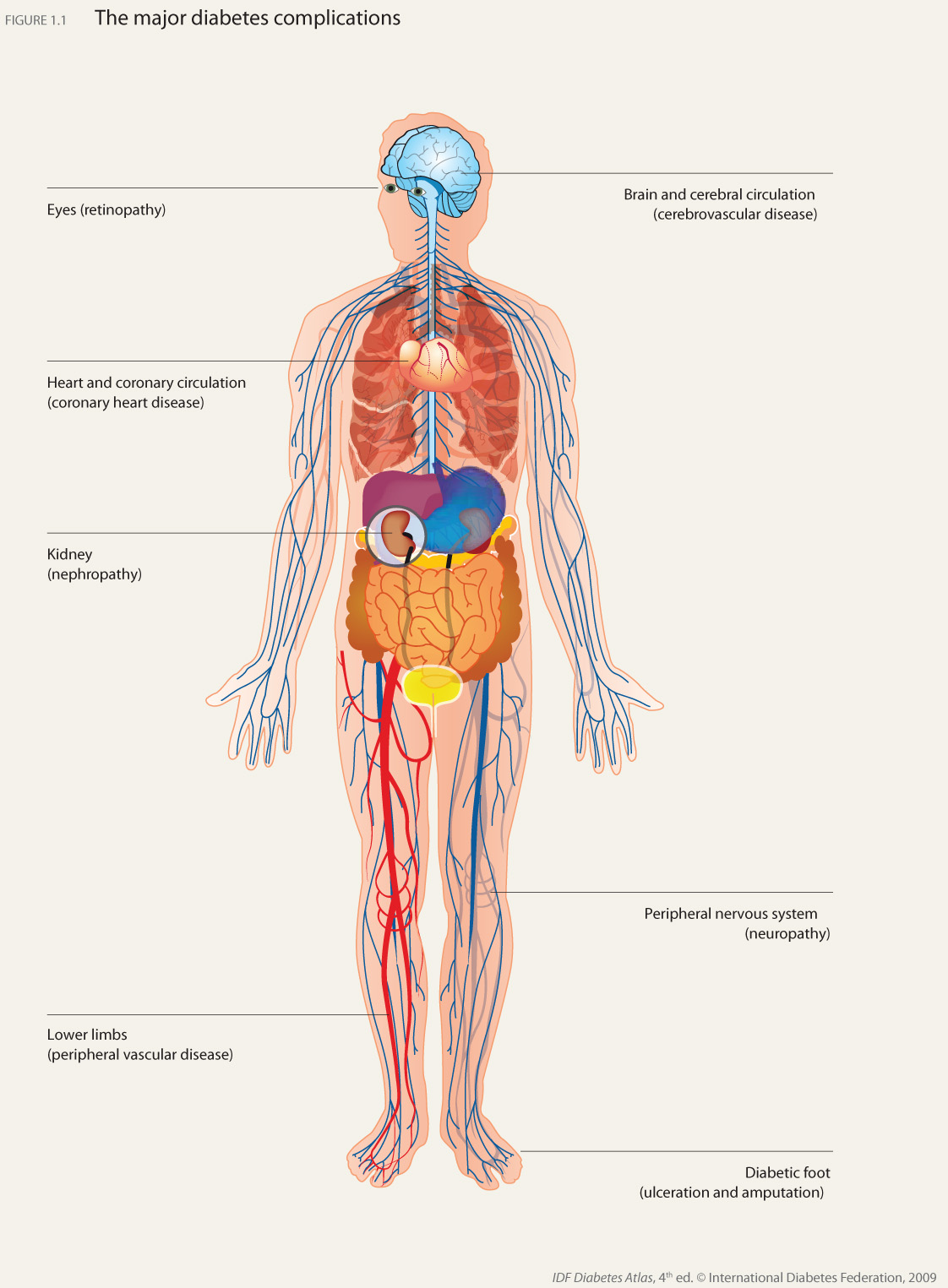
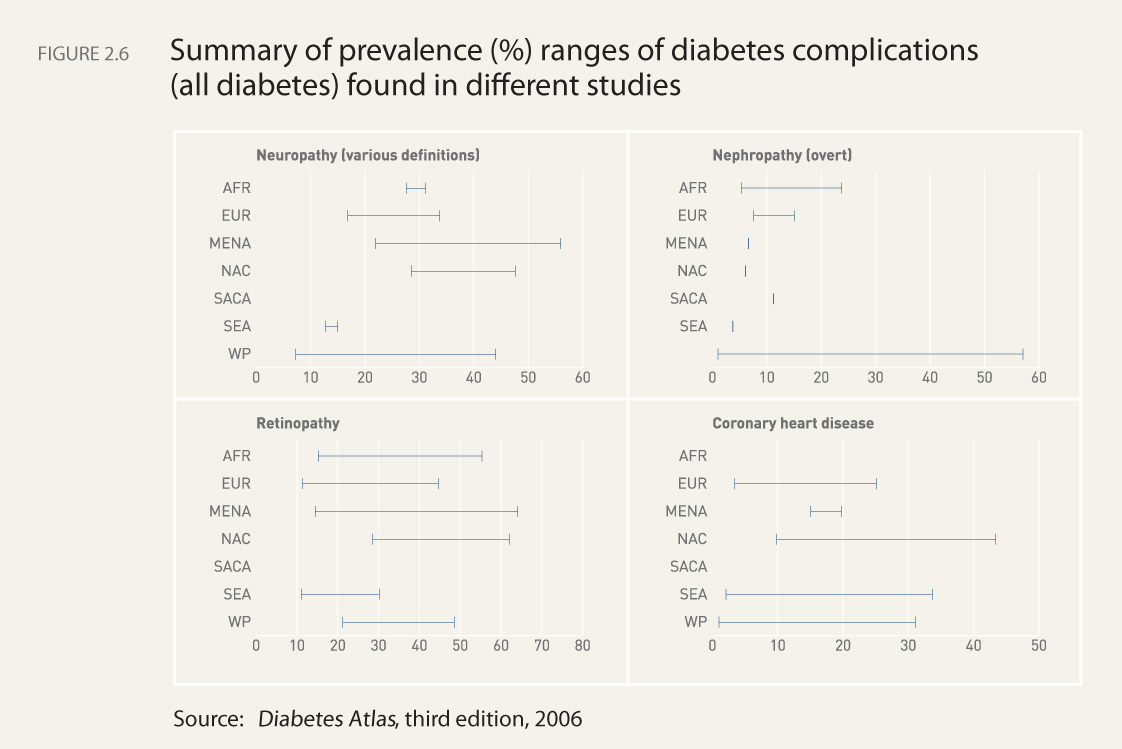
Diabetes mellitus (DM) is now one of the most common non-communicable diseases globally. It is the fourth or fifth leading cause of death in most high-income countries and there is substantial evidence that it is epidemic in many economically developing and newly industrialized nations. Complications from diabetes, such as coronary artery and peripheral vascular disease, stroke, diabetic neuropathy, amputations, renal failure and blindness are resulting in increasing disability, reduced life expectancy and enormous health costs for virtually every society. Diabetes is undoubtedly one of the most challenging health problems in the 21st century.
The number of studies describing the epidemiology of diabetes over the last 20 years has been extraordinary. It is now recognized that it is the low- and middle income countries (LMCs) that face the greatest burden of diabetes. However, many governments and public health planners still remain largely unaware of the current magnitude, or, more importantly, the future potential for increases in diabetes and its serious complications in their own countries.
It has been a consistent finding of population-based diabetes studies that a substantial proportion of all people found to have diabetes had not been previously diagnosed. The uncovering of new cases when mass blood testing is undertaken is primarily because of the lack of symptoms associated with the early years of type 2 diabetes, meaning that those with diabetes may be unaware of their condition and therefore not seek medical attention for it.
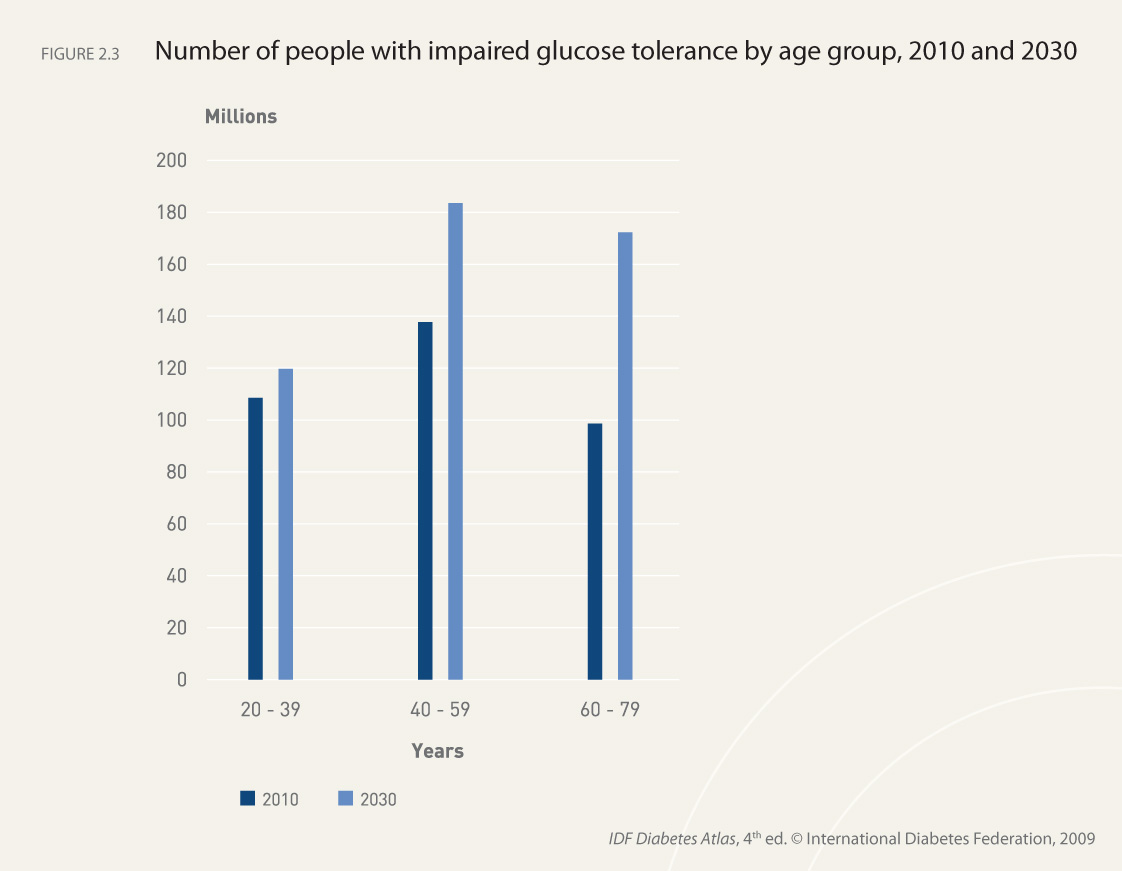
In addition to diabetes, the condition of impaired glucose tolerance also constitutes a major public health problem, both because of its association with diabetes incidence and its own association with an increased risk of cardiovascular disease.
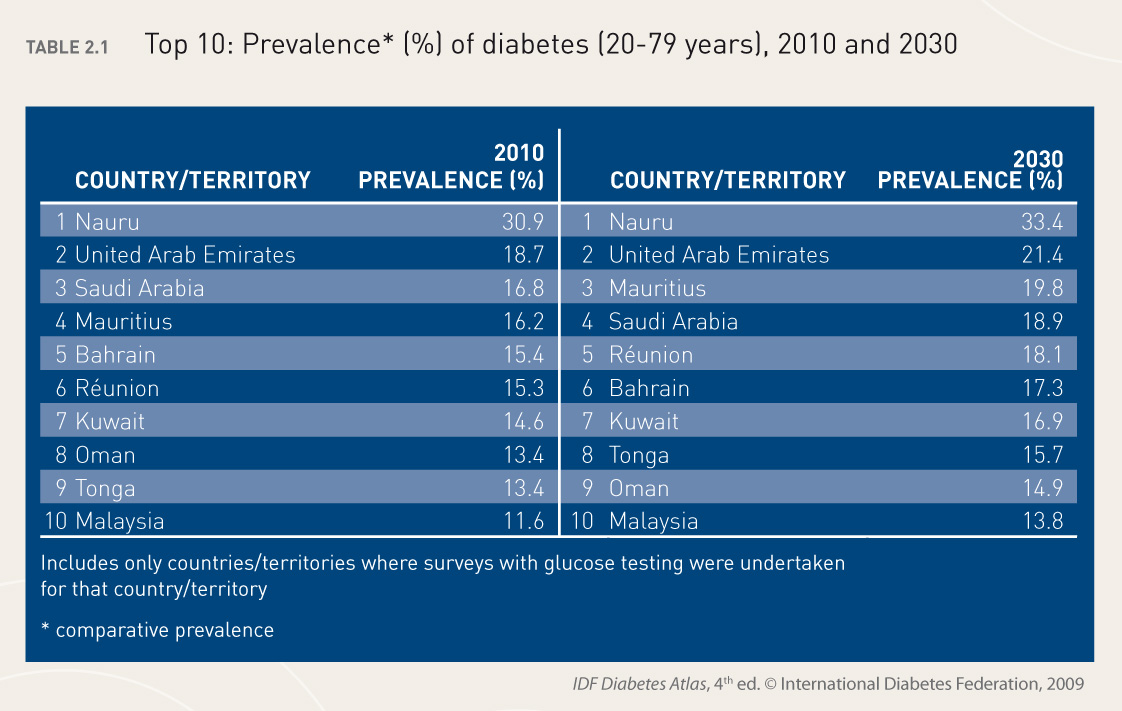
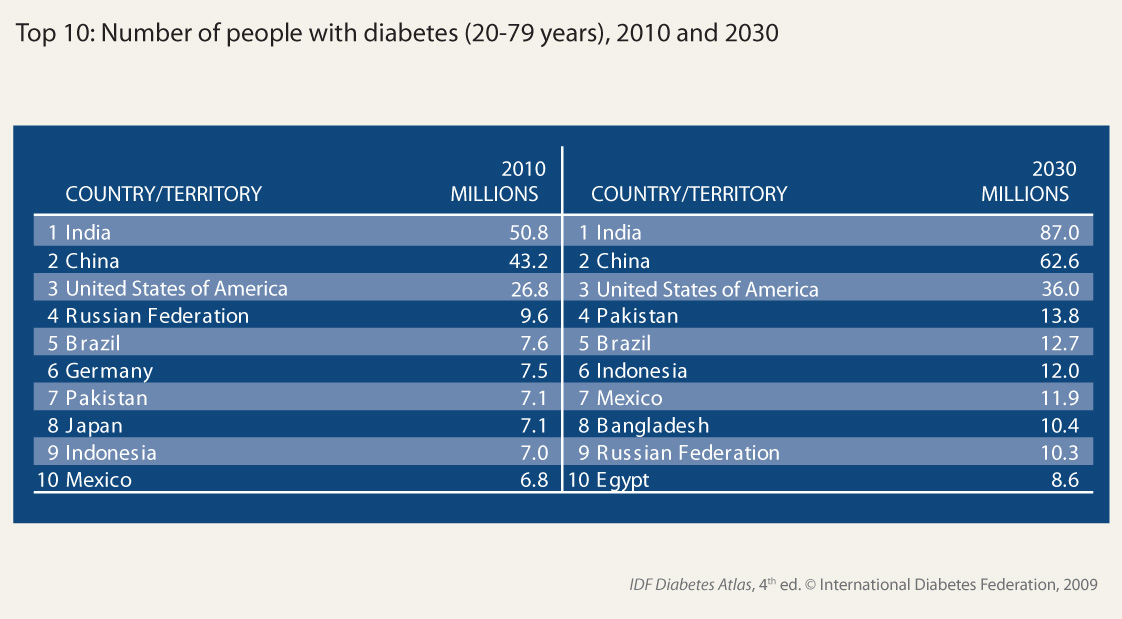
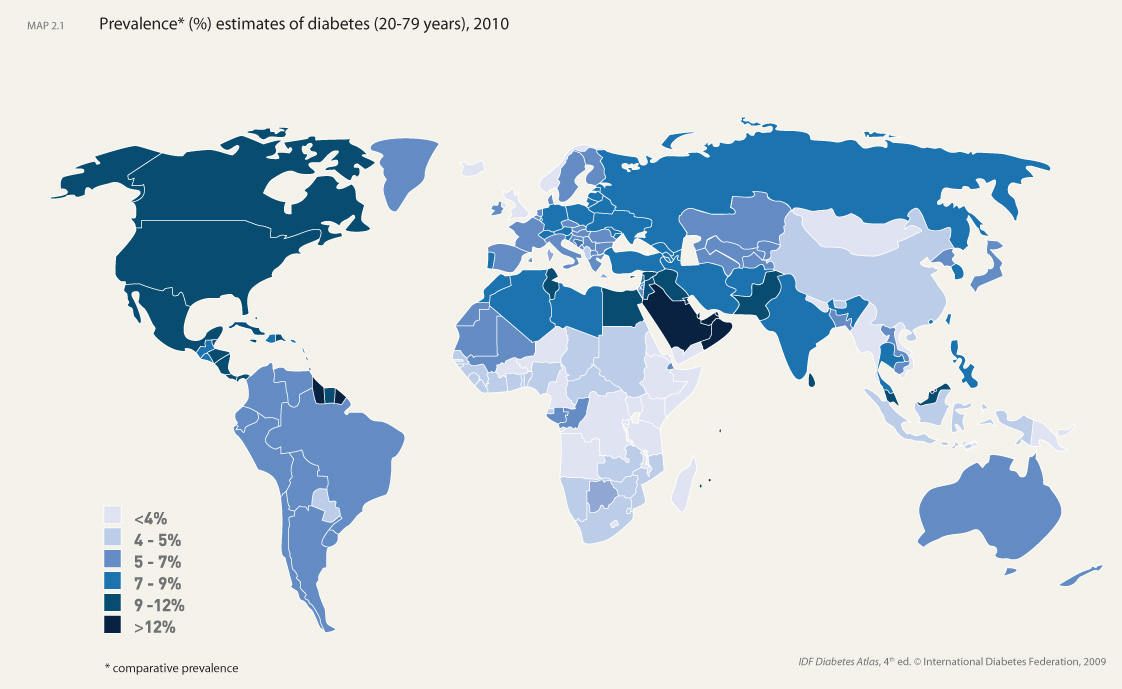
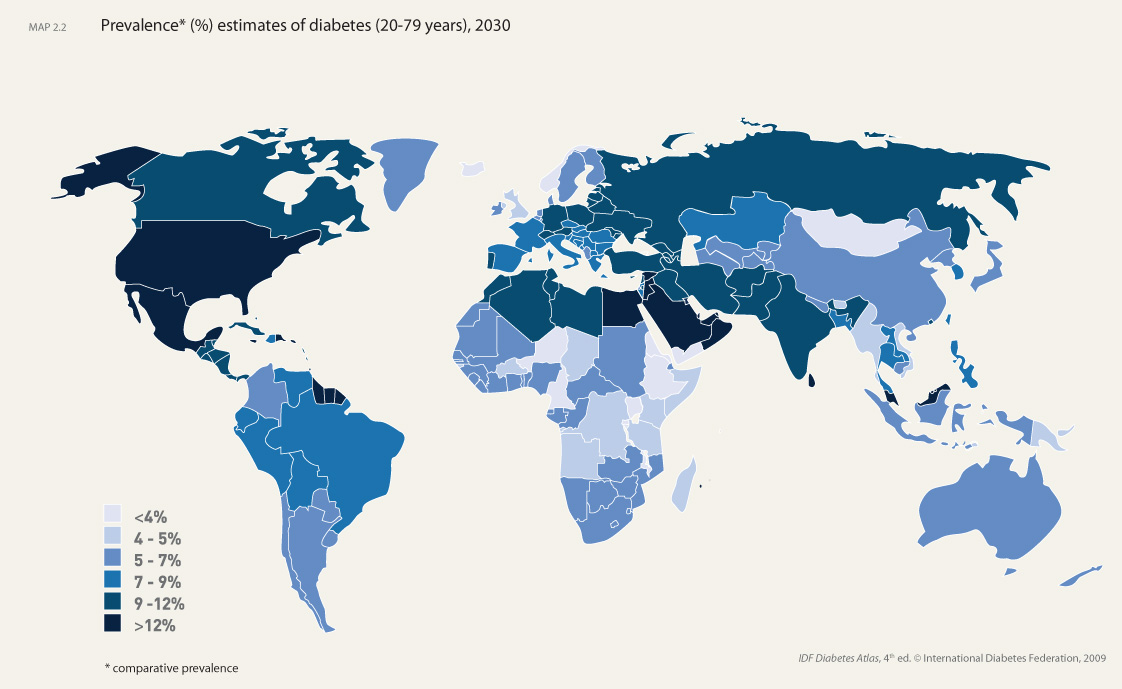
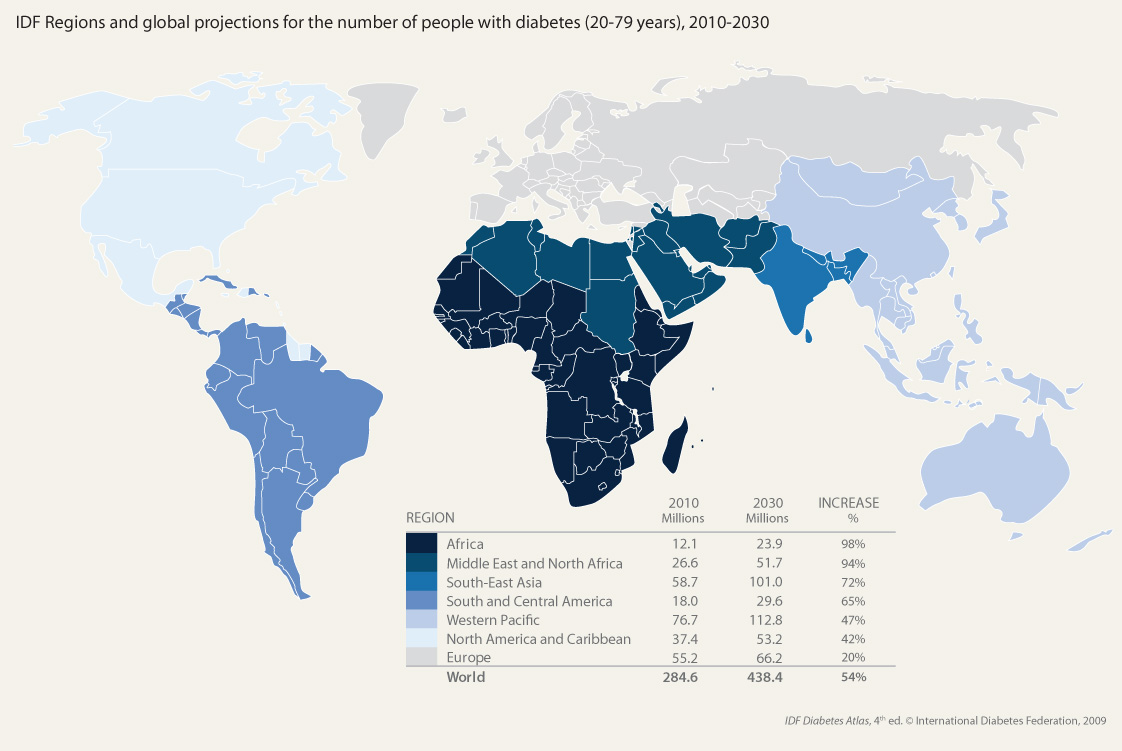
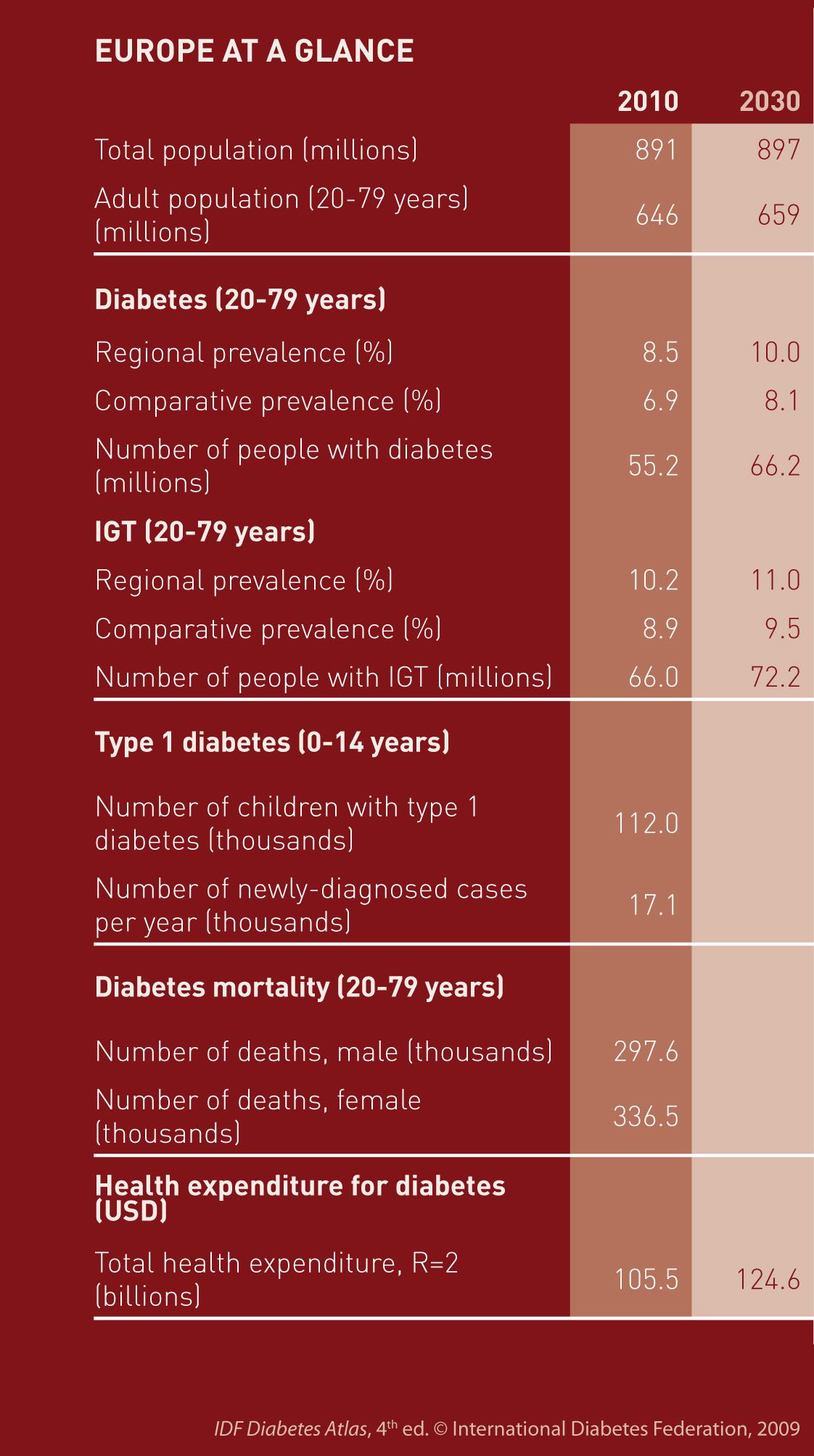
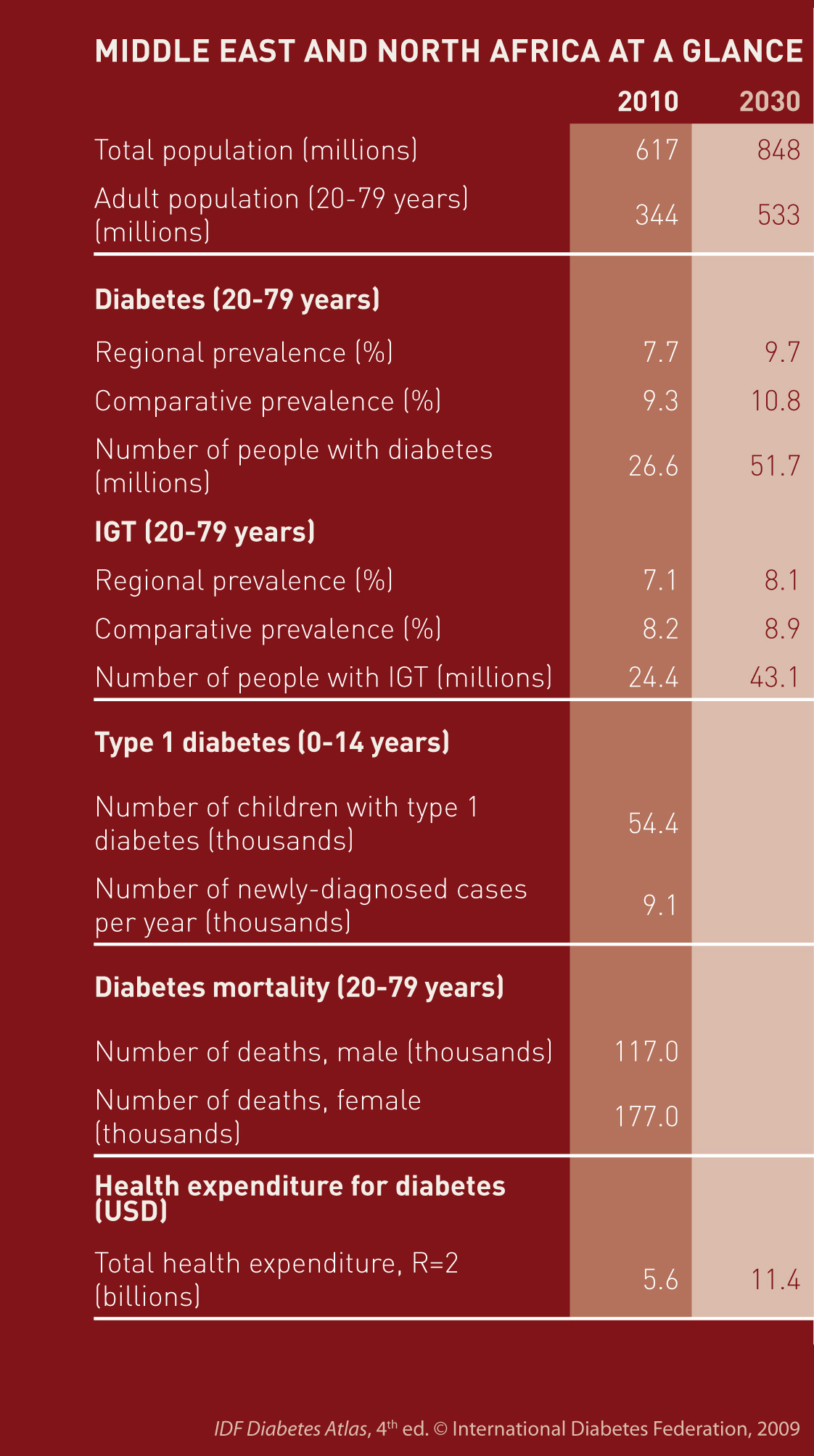
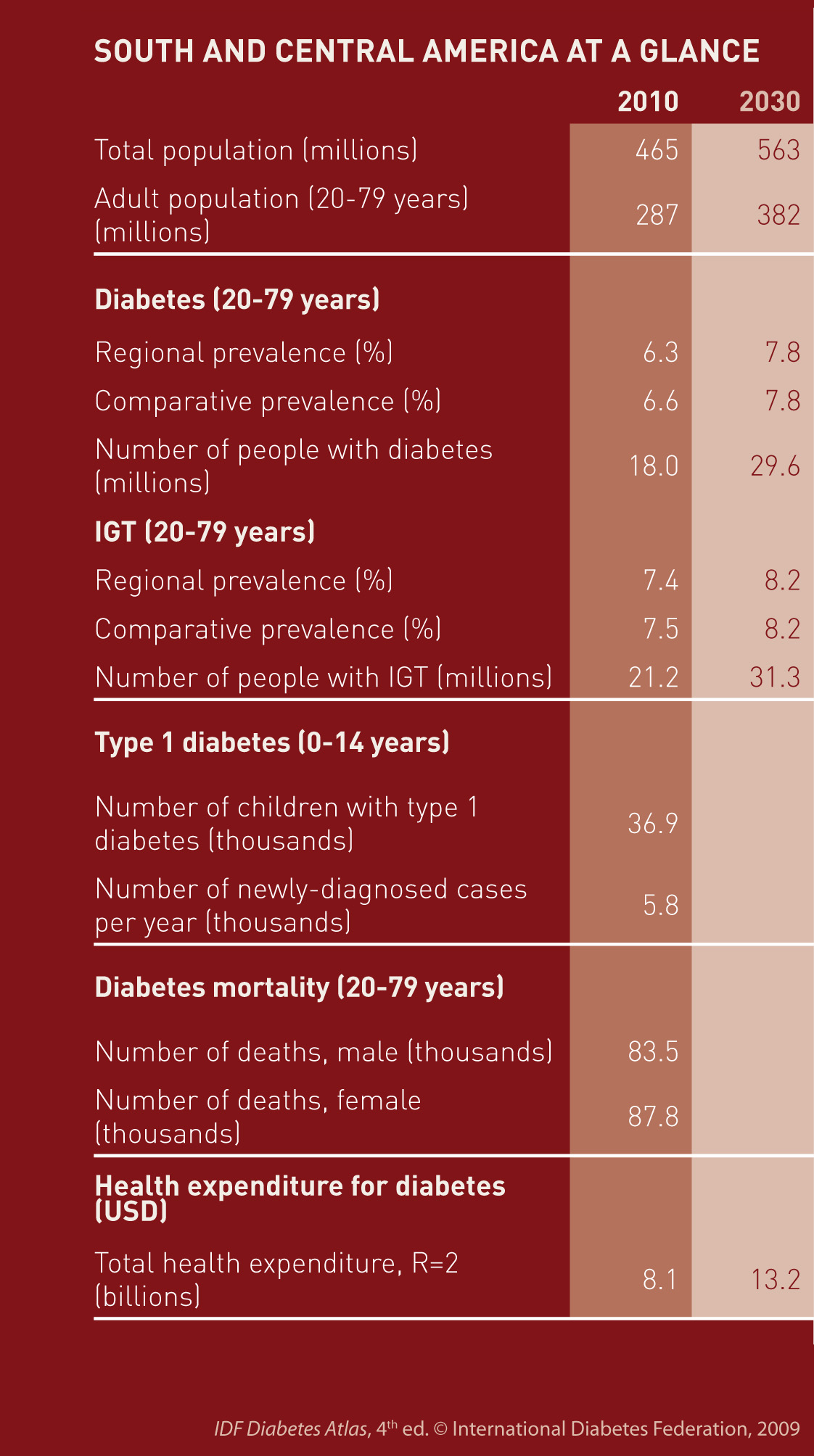
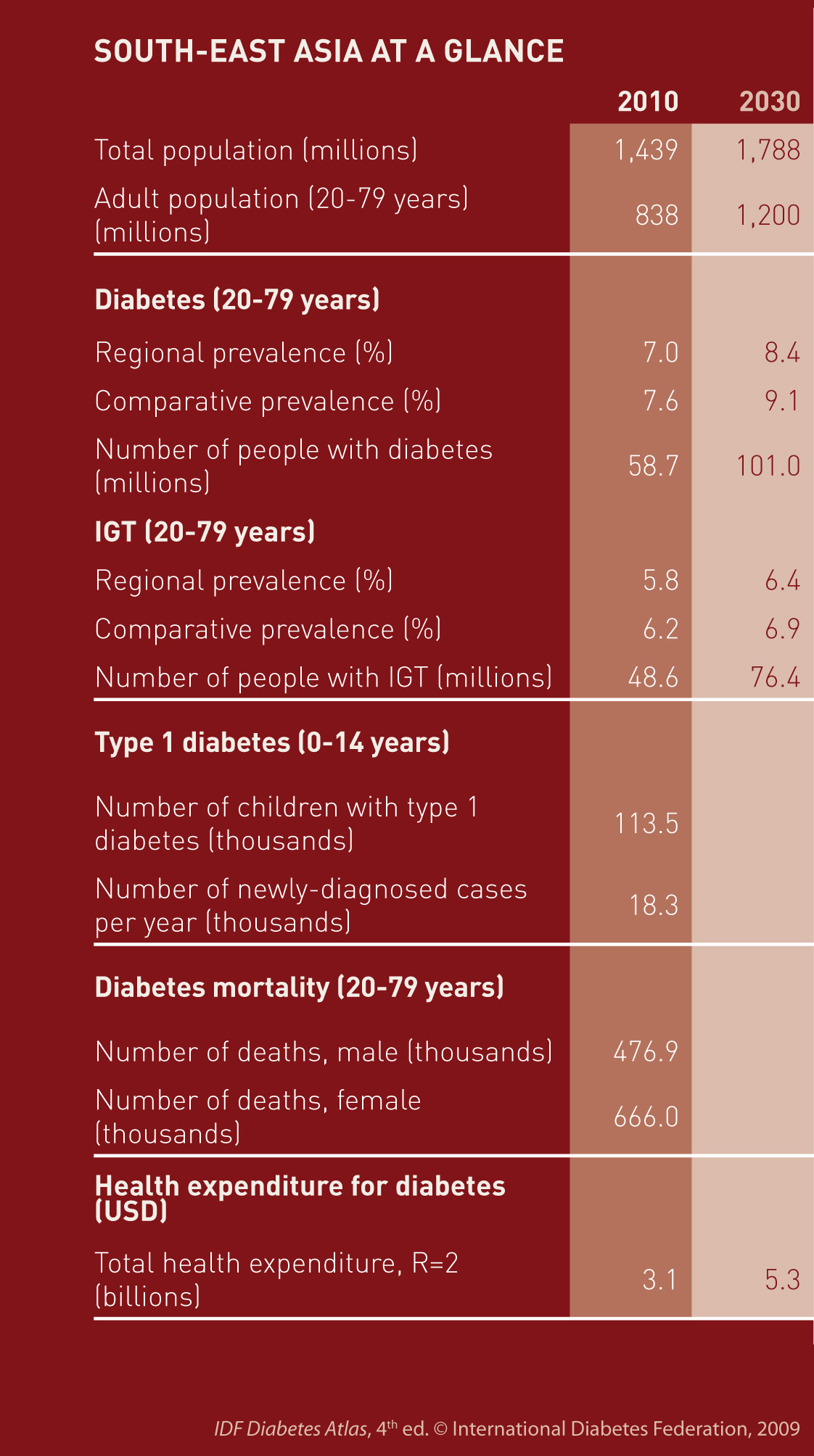
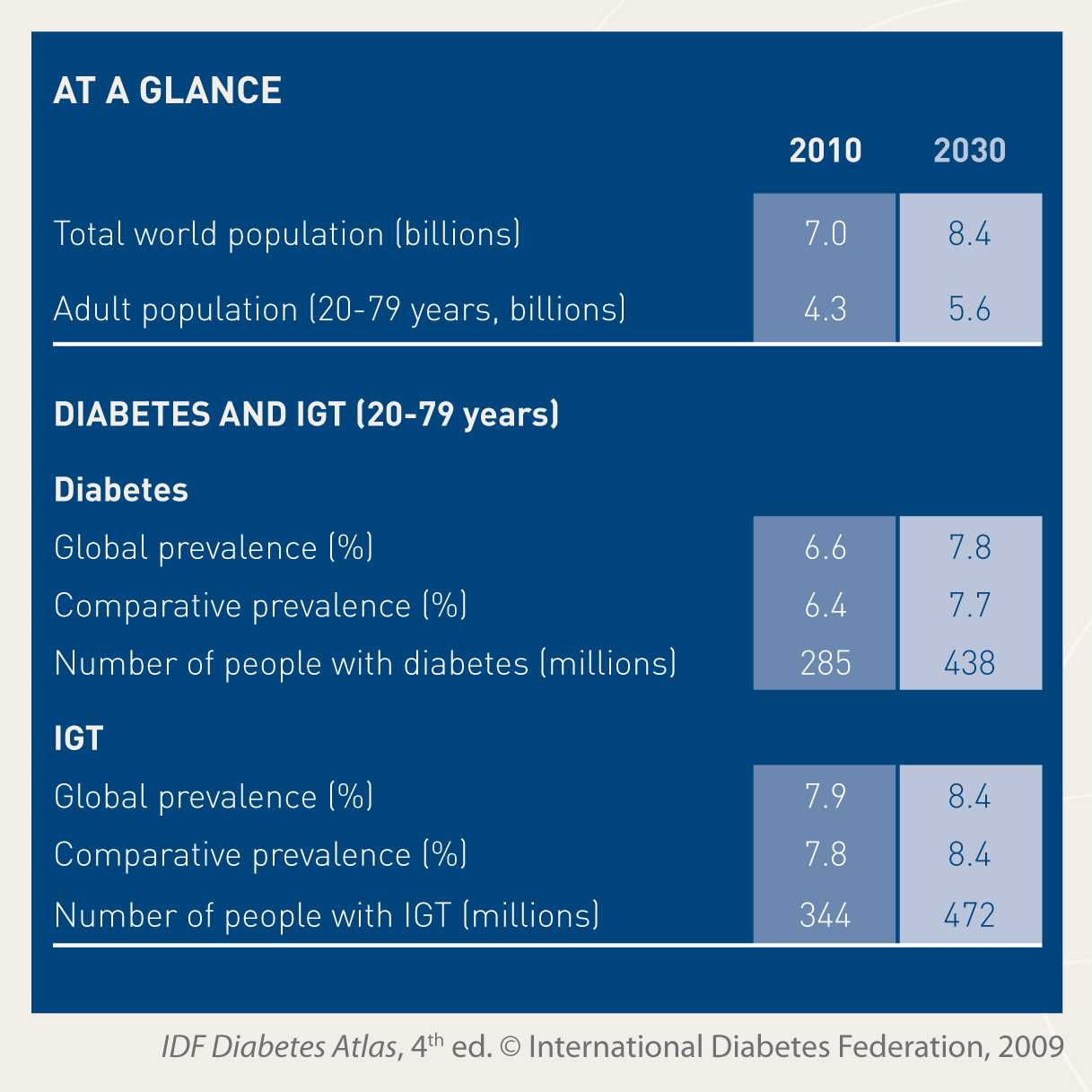
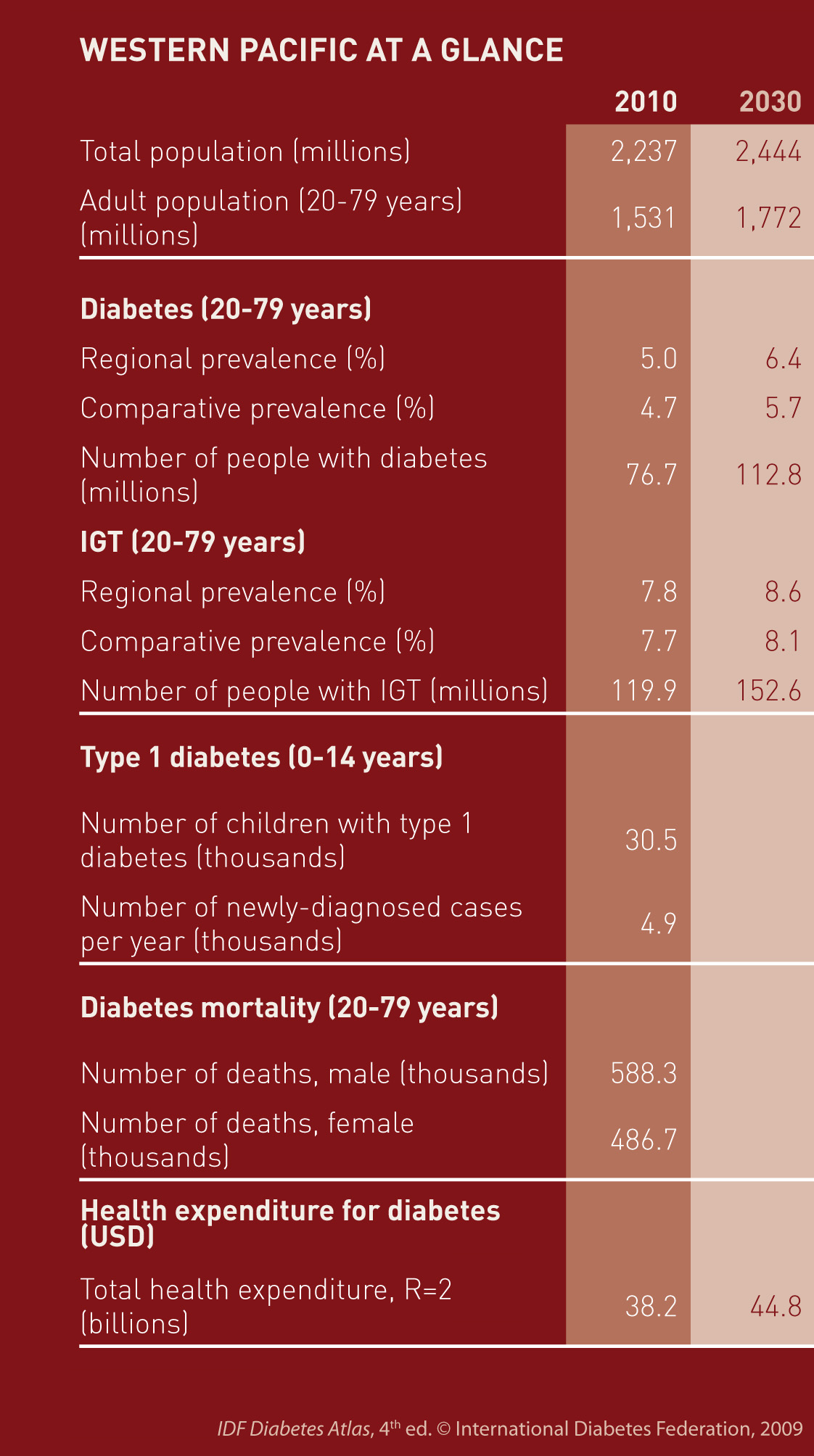
In this edition of the IDFDiabetes Atlas, the prevalence of diabetes mellitus and IGT has been estimated for each country for the years 2010 and 2030. Data are provided for 216 countries and territories, which have been allocated into one of the seven IDF regions: Africa (AFR), Europe (EUR), Middle East and North Africa (MENA), North America and Caribbean (NAC), South and Central America (SACA), South-East Asia (SEA), and the Western Pacific (WP).
The data presented for adults are for types 1 and 2 diabetes combined, and IGT. Only adults aged from 20 to 79 years are considered because the majority of all people who have diabetes and IGT are adults. Estimates for type 1 diabetes in children and adolescents are presented in the section on Diabetes in the Young.
Two sets of prevalence estimates have been provided in this report: the national, regional or global prevalence (the crude prevalence) and the comparative prevalence. The national, regional or global prevalence indicates the percentage of a particular population that has diabetes. It is appropriate for assessing the burden of diabetes for each country or region. The comparative prevalence is used for making comparisons between countries or regions. It has been calculated by assuming that every country or region has the same age profile (the age profile of the world population has been used). This reduces the effect of the differences of age between countries or regions, and makes this figure approriate for making comparisons.
The data presented here should be interpreted cautiously as general indicators of diabetes frequency, and the estimates will need to be revised as new and better epidemiological information becomes available. Comparison of country, regional, and even global prevalence from one report to the next should be performed with extreme caution. Large changes in the prevalence or numbers of people with diabetes from one edition of the IDF Diabetes Atlas to another are usually due to the use of a more recent study rather than a change in the profile of diabetes within that country. Data sources for this edition include 34 new studies. Thus, the inclusion of recent, and more reliable research brings us closer to the actual rates of diabetes, but these limitations need to be always considered. The key purpose of reports such as these is to stimulate action in the form of preventive and management programmes, as well as further research.
The background paper, Diabetes and Impaired Glucose Tolerance, and country by country estimates on which this summary is based are available in the Downloads section.
'Het verlangen om medicijnen in te nemen is misschien het belangrijkste verschilpunt tussen de mens en het dier.' (Sir William Osler (1849-1919))
Blijf altijd op de hoogte van de ontwikkelingen op KimTube.nl. Krijg als eerste te horen wanneer er nieuwe filmpjes van Kim en haar geile vriendinnen online zijn!
klik Gratis Kim Holland Film en vul jouw email-adres in en je krijgt een gratis Kim Holland film kado!





 The background paper, Diabetes in the Young, and country by country estimates on which the summary on type 1 diabetes in the young is based are available in the
The background paper, Diabetes in the Young, and country by country estimates on which the summary on type 1 diabetes in the young is based are available in the 
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}